The opioid epidemic and its associated overdose deaths have been widely reported in the past few years. In response, the Center for Disease Control issued a guideline for prescribing opioids for chronic pain (excluding cancer, palliative and terminal pain) in March 2016. The guidelines were developed to reduce inappropriate prescribing practices with a goal of reducing opioid use disorder, overdoses and death.
One focus was reducing the dosage and the duration of opioid treatment to the minimum necessary to relieve pain. It suggested that three days of treatment is often sufficient for the relief of pain, with more than seven days rarely being needed. The guidelines encouraged the discussion of the dangers of overdose between physicians
and patients on long-term, high-dose treatments. The question arises, are there signs of
benefit?
There is an unavoidable lag time to collect data on prescriptions written and reported
deaths due to overdose. However, preliminary data is encouraging. The prescribing of
opioids peaked in 2012 with a rate of 81.3 opioid prescriptions per 100 persons in the US.
The prescription rate in 2017 was down to 58.7 per 100, the lowest in a decade. There
are still pockets of very high prescribing rates in the US with 16% of counties reporting
enough prescriptions for every person to have had one.
The Impact of Fentanyl
Overdose death rates appear to be linked to prescription opioid exposure and appear to be related to the availability of illicit fentanyl. Fentanyl is a synthetic opioid that is approximately 100 times more potent than morphine and 50 times more potent than
heroin. Illegal fentanyl is often mixed into heroin or pressed into pill forms that mimic prescribed opioids. Slight miscalculations in illicit formulation can lead to overdose and death. Unfortunately, the number of fentanyl encounters collected by the DEA has increased dramatically (Figure 1).
FIGURE 1 - Regional Trends in Fentanyl Usage (Reported per 100,000 persons aged 15 or older, January 2001 - December 2016)
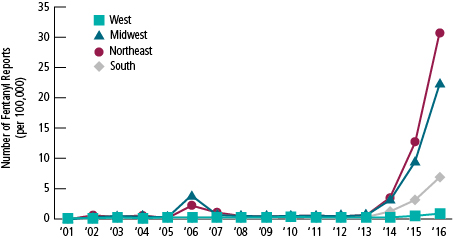
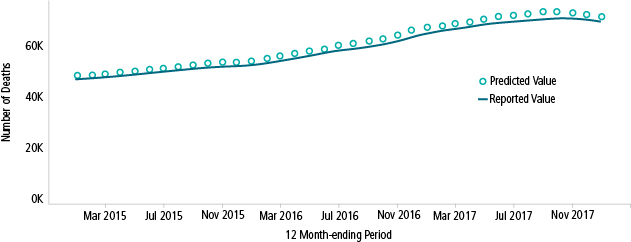
Interdiction of the flow of illicit fentanyl, treatment of opioid abuse disorder and awareness of the dangers of using illicit opioids are all important components of a solution to the problem of drug overdose deaths. The CDC monitors overdose deaths, and there may be the early beginnings of leveling off or improvement as shown in Figure 2.
FIGURE 2 - 12-month Ending Provisional Counts of Drug Overdose Deaths in US
Another encouraging opioid trend can be found in the Drug Testing IndexTM, a report on workforce drug positivity produced by Quest Diagnostics. Quest summarizes the prior year test results for their customers doing work-related employee drug testing. They found
that the opiate positivity rate in the general US workforce declined 17% from 2016 to 2017. Urine drug testing for heroin revealed a decline of 11% between 2016 and 2017 and hit a three-year low.
But the news from employee and pre-employee drug testing was not all good. The rate of positive urine cocaine tests had increased 7% in 2017 over 2016, marking the fifth year of
consecutive increases. Methamphetamine positivity also increased dramatically in certain areas of the country. Overall the combined drug positivity rate for the US workforce held steady year over year at 4.2% of specimens testing positive.
It does appear that efforts toward reversing opioid prescribing are beginning to have a positive effect, but continued programs to prevent overdose are needed. And ongoing monitoring of the situation is required.
References