A 36-year-old male applies for life insurance. He states that he is in good health except for a history of Hereditary Multiple Exostoses. He sees an orthopedic surgeon yearly. His mother also has this diagnosis and is alive and well. He has had two surgeries for removal of benign lesions in his knee and elbow.
Definition
Hereditary Multiple Exostoses (HME) is an autosomal dominant condition characterized by abnormal growth of long bones mainly affecting the epiphyses. Its many synonyms include Multiple Osteochondromas (MO), Multiple Hereditary Exostoses (MHE), EXT, Multiple Hereditary Osteochondromas (MHO) and Multiple Cartilaginous Exostoses.
Osteochondral growths (exostoses or osteochondromas), consisting of bone surrounded by a cap of cartilage, occur on the periphery of long bones. The patient must have two or more exostoses on the appendicular or axial skeleton to fulfill the definition of HME. Approximately 80% of individuals with this condition have a positive family history.
The major complaints of these patients are cosmetic deformities, pain and difficulty moving the joints. Osteochondromas are benign lesions that do not affect life expectancy. Rarely, these exostoses may transform into chondrosarcomas.
Presentation
The presentation often occurs in the second decade of life. Often it is an incidental finding, with males more than females. Incidence is estimated to be 1:50,000. The most common location is around the knee or the proximal humerus.
The osteochondroma can present as a painless mass or a painful mass with minimal trauma. The lesions can cause pain, decreased range of motion, deformity or pathologic fracture. The growth plates can be affected, with resultant short stature or angular deformities. Fifty percent of patients present with a clinically visible tumor by age 5, 80% by age 10. The average number of exostoses per patient is six.
Imaging
The best form of imaging for this is plain radiographs in at least two planes.
Figure 1 - Osteochondroma of distal femur
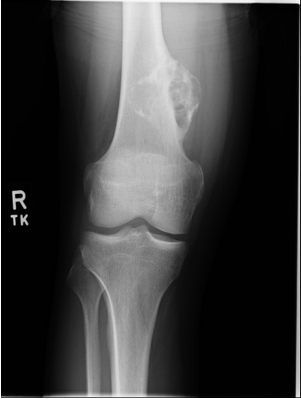
Accessed August 13, 2018 from Bing images, free to share and use
Genetics
HME is an autosomal dominant condition with 95% penetrance. Two EXT genes account for 90% of the lesions. EXT1 is located on the distal end of chromosome 8, and EXT2 is located on chromosome 11. EXT1 and EXT2 have been associated with both familial hereditary exostoses and spontaneous multiple hereditary exostoses.
Mutations in either of these genes result in clinically indistinguishable exostoses. The proteins resulting from EXT1 and EXT2 are glycosyltransferases, which catalyse heparin sulphate polymerization and appear to be a complementary pair that form a stable enzyme complex in vivo. Research has suggested that the EXT genes function as tumor suppressor genes.
Treatment
Treatment is generally supportive. Surgery is required for the management of pain and deformation. Also, monitoring is necessary for the possibility of malignant transformation of lesions to secondary chondrosarcomas. This occurs in approximately 0.5% to 5% of lesions, so yearly radiographs are advised. The five-year survival of a chondrosarcoma is 90%. A wide surgical excision is the treatment of choice.
Prognosis
Chondrosarcomas are benign and do not affect the life span of an individual. There is a low incidence (0.5% - 5%) of transformation to malignant lesions. These lesions have a five-year survival rate of 25-90%, depending upon location.
Malignant transformation occurs most often in osteochondromas of the spine, scapula, pelvis and proximal femur. Benign lesions generally have cartilage caps greater than two centimeters thick in adults and tend to stop enlarging when the bony growth plates close.
Returning to the Case
This gentleman has a history of HME and has yearly follow ups with his orthopedic surgeon. His mortality risk appears to be low to near standard.
References
- Bovée, Judith VMG. “Multiple osteochondromas.” Orphanet journal of rare diseases 3.1 (2008): 3.
- Porter, D. E., et al. “Severity of disease and risk of malignant change in hereditary multiple exostoses: a genotypephenotype study.” The Journal of bone and joint surgery. British volume 86.7 (2004): 1041-1046.
- Ryckx, Andries, J. F. Somers, and Lieven AllAeRt. “Hereditary multiple exostosis.” Acta Orthop Belg 79.6 (2013): 597-607.
- Schmale, Gregory A., Ernest U. Conrad, and Wendy H. Raskind. “The natural history of hereditary multiple exostoses.” JBJS 76.7 (1994): 986-992.
-
www.uptodate.com last accessed 8/13/2018